
 English
English
 French
French
 Pubmed
Pubmed Google Scholar
Google Scholar Cross Ref
Cross Ref Visistor: 1701582
Visistor: 1701582 Damage control in the management of severe penetrating chest trauma.
Le contrôle des dommages dans le traitement des traumatismes thoraciques pénétrés graves.
S. Rabiou1, I. Oughebbi2, K. Sidibe3, P. Nyat4, J. Ghalimi1, Y. Ouadnouni1,5, A. El Bouazzaoui4,5, M. Smahi1,5.
1: Department of Thoracic Surgery, University Hospital Hassan II-Fez, Morocco.
2: Departement of Cardiovascular Surgery, University Hospital Hassan II-Fez, Morocco.
3: Departement of radiology, University Hospital Hassan II-Fez, Morocco.
4: Departement of Anesthesia and Resuscitation. University Hospital Hassan II-Fez, Morocco".
Corresponding author
Dr. Sani RABIOU
Service de Chirurgie Thoracique. CHU Hassan-II, Fès, Maroc
E-mail: rabiousani2@yahoo.fr
ABSTRACT
Penetrating chest injuries are responsible for a high mortality due to hemorrhagic shock they generate. The management of these patients must be done according to the principle of Damage control. The rapid control of bleeding by minimalist surgery, remains the cornerstone of this management. The collaboration between surgeon, intensivist, anesthesiologist and radiologist is a critical element determining the patient’s prognosis. We reoport a case of a yong patient was admitted to the emergency room after a violent car crash with a violent penetrating chest trauma.
KEYWORDS: Chest Trauma, penetrating chest wound, damage control.
RÉSUMÉ
Les traumatismes thoraciques pénétrants sont responsable d'une mortalité élevée liée aux choc hémorragique qu'ils engendrent. La prise en charge de ces patients doit répondre à des impératifs qui correspondent au principe de Damage control. Le contrôle rapide de l' hémorragie, au moyen d'une chirurgie à minima, demeure la pierre angulaire de cette prise en charge. La collaboration entre chirurgien, urgentiste, réanimateur et radiologue est un élément essentiel déterminant le pronostic du patient. Nous rapportons le cas d'un jeune patient admis aux urgences suite à un violent accident de la voie publique ayant occasionné un traumatisme thoracique pénétrant dont la prise en charge avait nécessité la tactique de Damage control.
MOTS CLÉS: Traumatisme thoracique, plaie thoracique pénétrante, control des domages.
INTRODUCTION
Penetrating chest injuries are responsible for a high mortality due to hemorrhagic shock they generate. The management of these patients must be done according to the principle of Damage control. The rapid control of bleeding by minimalist surgery, remains the cornerstone of this management [1]. The collaboration between surgeon, intensivist, anesthesiologist and radiologist is a critical element determining the patient’s prognosis.
CASE HISTORY
A 34 year old male was admitted to the emergency room after a violent car crash with a violent penetrating chest trauma. Clinical examination found a large wound in the chest wall at the second left intercostal space exposing a portion of the upper lobe of the left lung that was ventilating outside the thorax (Figure 1).
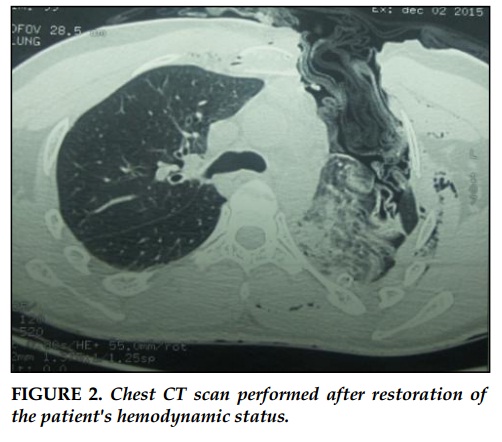
There was also a hemorragic shock with high heart rate and low arterial pressure. Before this hemodynamic and respiratory instability the patient had been immediately taken to the operating room without any previous tests. Surgical exploration had found mediastinal hematoma with a contusion of the left subclaviar vessels associated with significant sagging chest wall which was bleeding. After obtaining a satisfactory hemostasis with restoration of hemodynamic status, intubated and ventilated patient was taken to the radiology department where a chest CT scan was performed (Figure 2).
After the readmission into the operating room a second operation look had allowed the repair of lesions with satisfactory parietal repairs. Post operative surveillance in an intensive care unit during the next six days was satisfactory with respiratory and hemodynamic stability.
DISCUSSION
The Damage Control concept remains the standard of care in war medecine. It follows the concept of Damage Control Surgery or shortened surgery which effectiveness had been established in patients with severe trauma with hemodynamic disorder endangering the vital prognosis and making a long surgery too risky [2]. In these patients with hemodynamic instability, the first imperative is speed: speed to address and place the patient in the operating room for rapid achievement of hemostasis.
The need for this quick intervention becomes evident when in an uncompensated hemorrhagic shock which may at any time cause cardiac arrest. The speed of the initial surgical procedure is also essential in a large hemorrhagic injury to avoid the appearance of lethal triad of Moore associating: hypothermia, acidosis and coagulopathy [3].
As pointed in our case, prevention of this triad comes with the appliance of the so-called damage control tactic , which involves treating the wounded in three stages: first fast surgery, that should not exceed 1h to 1h30, referring only to hemostasis, second stage with resuscitation when the constants are restored (patient warming, transfusion and correction of coagulopathy, fight against acidosis ) and a third time implying a definitive surgical repair when these constants have been restored (12-48 hours after the first intervetion).
CONFLIT OF INTEREST
There are no conflicts of interest.
REFERENCES
1. Shapiro MB, Jenkins DH, Schwab CW, et al. Damage control: collective review. J Trauma 2000; 49:969-78.
2. Kauvar DS, Wade CE. The epidemiology and modern management of traumatic hemorrhage: US and international perspectives. Crit Care 2005; 9(5):1–9.
3. Shapiro MB, Jenkins DH, Schwab CW, Rotondo MF. Damage control: collective review. J Trauma 2000;49:969–78.

FIGURES

REFERENCES
1. Shapiro MB, Jenkins DH, Schwab CW, et al. Damage control: collective review. J Trauma 2000; 49:969-78.
2. Kauvar DS, Wade CE. The epidemiology and modern management of traumatic hemorrhage: US and international perspectives. Crit Care 2005; 9(5):1–9.
3. Shapiro MB, Jenkins DH, Schwab CW, Rotondo MF. Damage control: collective review. J Trauma 2000;49:969–78.
ARTICLE INFO
DOI: 10.12699/jfvp.7.21.2016.48
Conflict of Interest
Non
Date of publication after correction
18/7/2016
Article citation
Rabiou S , Oughebbi I, Sidibe K, Nyat P, Ghalimi J, Ouadnouni Y, El Bouazzaoui A, Smahi M. Damage control in the management of severe penetrating chest trauma. J Func Vent Pulm 2016; 21(7): 48-50.



Copyright: jfvpulm.com