
 English
English
 French
French
 Pubmed
Pubmed Google Scholar
Google Scholar Cross Ref
Cross Ref Visistor: 1711136
Visistor: 1711136Study on the impact of CO2 inflation on cardiorespiratory system in patients having endoscopy surgery
Étude de l'impact de CO2 gonflement sur le système cardio-respiratoire chez les patients ayant la chirurgie endoscopique
T. Le Van, H. Ta Thanh
Hai Duong Medical Technical University. Hai Duong, Viet Nam
Corresponding author
Docteur LE VAN Them
Hai Duong Medical Technical University. Hai Duong. Viet Nam
Email : themlv2003@gmail.com
ABSTRACT
Objective. To describe the change of heart rate (HR), respiratory rate, and blood pressure in patients with abdominal endoscopic anesthesia surgery when CO2 pumps into peritoneal cavity.
Methods. It was a perspective and descriptive study.
Results. HR strongly decreased from T5 to T25, average HR minimum was at T20; HR was decreased from 76.85±7.630 to 67.05±10.396 beats/min or by 12.75% reduction. In our study, 19 patients with HR was decreased to 51-59 beats/min; 15 patients with HR was decreased to ≤ 50 beats/min. In those patients with HR ≤50 beats/min, Atropin 10mcg/kg was used with good outcome. HR of patients after exhaust gas tented to gradually increase and stable toward the value of LM period. Blood pressure during CO2 pumps in 20 first minutes was increased. Average blood pressure maximum at T5 from 84.13±7.489 to 93.78±9.703 or by 11.47%. Blood pressure was slightly increased and stable from T25 to T120. After CO2 exhaust, blood pressure was slightly increased then toward it was before surgery but less than that. There was no change in respiratory rate.
KEYWORDS: CO2 pump, heart rate, blood pressure, respiratory rate, endoscopic surgery.
RÉSUMÉ
Objectif. Pour décrire l'évolution de la fréquence cardiaque (FC), fréquence respiratoire et de la pression artérielle chez les patients ayant subi une chirurgie abdominale endoscopique lorsque le CO2 est soufflé dans la cavité péritonéale.
Méthodes. Il s’agit d’étude descriptive en perspective.
Résultats. FC a été fortement diminué de T5 à T25, FC minimum moyen à T20; FC diminuait de 76,85±7,630 à 67,05±10,396 battements/min ou de 12,75% de réduction. Dans notre étude, 19 patients avec FC ont été diminué à 51-59 battements/ min; 15 patients avec FC ont été diminué à <50 battements/min. Chez les patients présentant une FC <50 battements/min, l’Atropin à 10 µg / kg a été utilisé avec un bon résultat. FC des patients après que les gaz d'échappement ont été amenés à augmenter progressivement et à se stabiliser vers la valeur de la période LM. La pression artérielle pendant les 20 premières minutes de CO2 a été augmenté, la pression artérielle au T5 le plus élevé étant passée de 84,13±7,489 à 93,78±9,703 ou à 11,47%. La pression artérielle a été légèrement augmenté et stable de T25 à T120. Après l’échappement du CO2, la pression artérielle a éýe légèrement augmenté vers celle avant l’intervention mais plus petite. Il n’y avait pas de changement pour la fréquence respiratoire.
MOTS CLÉS: CO2 gonflement, fréquence cardiaque, fréquence respiratoire, chirurgie endoscopique.
INTRODUCTION
Laparoscopic surgery is considered to be a surgical revolution that has been used in diagnostics and treatment since the late 1980's and has been widely used in a variety of ways. In the field of obstetrics, gastrointestinal diseases, urology, chest, .... Laparoscopic surgery has advantages over open surgery: less traumatic surgery, short hospital stay, minimally invasive surgery, less postoperative pain, significantly reduced complications of bacterial infection and adhesion after surgery, ensure aesthetics, recovery time after surgery faster [1].
Along with the advancement of laparoscopic surgery, anesthesia has many experimental and clinical studies related to laparoscopic surgery that have been conducted to address this issue. The use of CO2 pumps into the peritoneal cavity and extra-peritoneal cavity to expand the surgical site making the anesthetists to face the changes in circulation and respiration due to the pumping effect.
The understanding of these mechanisms is essential for application in the selection of the best anesthesia, monitoring, attitudes, and care for patients with endoscopic surgery. The circulatory and respiratory disorders, and body temperature are highly dependent on inflatable pressure, inflatable area (intra-peritoneal or non-peritoneal) and pumping time [2].
In addition, CO2 that is a cold gas when injected into the body over a long period of time can lead to hypothermia. The method of laparoscopic surgery has many advantages, but it causes many disorders for patients so the anesthesia workers must always focus on monitoring, care and coordination in time to solve. Ensure safety for patients [2].
There are some studies on the effect on circulation in patients with endoscopic cholecystectomy or ovarian cystoscopy. However, for other endoscopic surgeries, the level of respiratory, circulatory, and thermal effects is very high.
From the above situation we conducted the study on this topic with the aim to describe the changes in heart and respiratory rates and blood pressure in laparotomy with CO2 pumping into the peritoneal cavity.
METHODS
Study subjects
Patients undergoing laparoscopic surgery with CO2 pumping into the peritoneal cavity with anesthetic methods by endotracheal anesthesia such as: endoscopic cholecystectomy, endoscopic appendectomy, endoscopic surgery colonoscopy, endoscopic surgery for cystic ovaries, ... at the Surgery, Anesthesia and ICU Department of the Military Central Hospital 108.
Standard criteria of inclusion
Age ≥18
Patients did not have diseases such as heart failure, coronary heart disease, chronic valvular heart disease, chronic lung disease, emphysema, lung bulla, increased intracranial pressure, glaucoma.
ASA: I or II according to the classification of the American Anesthesia Association.
Inflated time ≤ 2h.
Patients agreed to participate in the study.
Exclusion criteria
Patients did not agree to participate in the study.
Patients did not have sufficient awareness to answer such as: syncope, mental disorder, deaf, ...
Methods
Study design
It was a propective and descriptive study.
Sample size and sampling methods
All included patients underwent peritoneal laparoscopic surgery with general anesthesia with endotracheal anesthesia method at the Surgery and Anesthesia Department of Military Central Hospital 108.
Time and place of study
Location: Department of Surgery and Anesthesia of Military Central Hospital 108.
Time: from April to June 2018.
Information gathering techniques
Sources of information: Medical records collected information on name, age, sex, diagnosis, indications of surgery, surgeon, surgery day, anesthesia method, anesthesiologist.
Observe, asking, examining the patient, and medical history, height, weight, …were made.
Assessment of cardio-respiratory changes (pulse, blood pressure, SpO2) was based on the monitoring of the indicators on the monitoring machine, the anesthesia machine at the time of the study and recorded on the data collection form.
Data processing and analysis
The results of present study were processed according to SPSS software 20.0 (Chicago; USA). Data are expressed as mean± SD, percentage (%).
RESULTS
General characteristics of patients and surgery
Of the 86 patients studied there were 37 patients were male accounting for 43.02%; 49 patients were female, accounting for 56.98%.
Age group: from 18 to 39 years old, there was 32 patients accounted for 37.21%; from 40 to 59 years old, there was 28 patients accounted for 32.56%; for ≥60 years old with 26 patients accounting for 30.23%.
ASA: there were 59 patients in ASA I accounting for 68.60%, 27 patients in ASA II accounted for 3.40% (Table 1).
BMI: 5 patients with low weight, 5 patients with obesity level 1 accounted for 5.81%; 16 pre-obesity patients accounted for 18.60%; 60 patients in the normal state accounted for 69.78%.
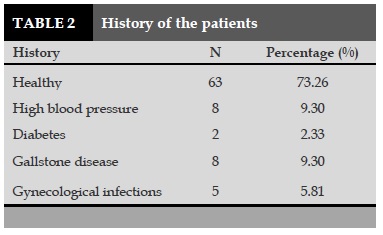
Of the 86 patients studied the majority of patients with a healthy history (73.26%), hypertension accounted for 9.30%, gallstones accounted for 9.30% (Table 2).
Five patients with a history of gynecological infections accounted for 5.81%.
2 patients with history of diabetes were accounted for 2.33%.
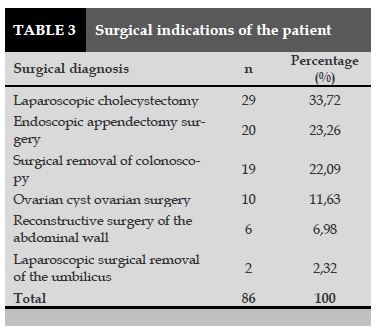
86 study patients there were 29 cases of laparoscopic surgical excision of gallbladder accounted for 33.72%, 2 patients of umbilical cord cystoscopy surgery, accounting for 2.32% (Table 3).
Changes in pulse and blood pressure of patients over time
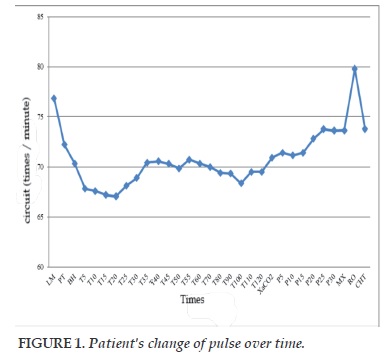
The pulse was decreased sharply from T5 to T25; lowest average pulse at time T20; the pulse was decreased from 76.85±7.630 to 67.05±10.396 times per minute or decreased 12.75%. From T30 to T120 the pulse was increased slightly and stabilized.
The pulse was increased slightly after discharge of CO2 at the time of extubation and the high pulse due to irritation, at the time of recovery, the pulse was in normal range.
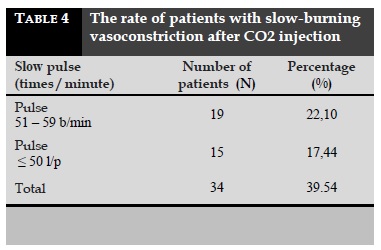
In 86 study patients, after the process of CO2 pumping into the peritoneal cavity, there were 34 patients falling below 60 b/min accounted for 39.54% of which: 19 patients with pulse from 51 to 59 b/min accounting for 22.10%.
Fifteen patients had pulse ≤50 b/min accounting for 17.44%. Patients with pulse ≤50 b/min were treated with intravenous Atropin 10mcg/kg and 100% effective immediately after the injection, patients’ pulse was returned to the normal range.
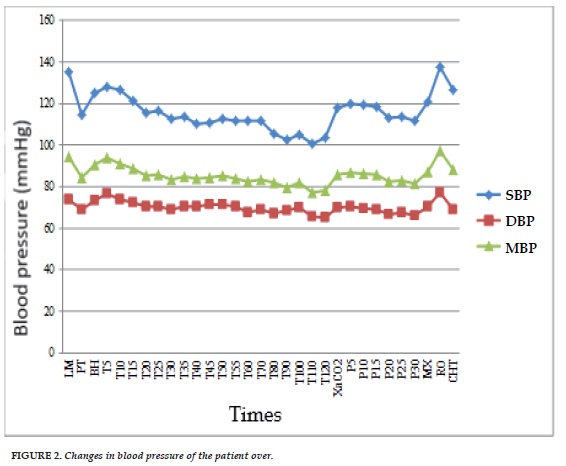
Maximum, mean, and minimum reduction in blood pressure at the time of surgery compared to baseline blood pressure was presented in Figure 2.
Since the CO2 inflating, blood pressure was rised, high blood pressure was increased between T5 to T20. Blood pressure was highest at time T5: systolic blood pressure (SBP) was increased from 114.62± 10,880 to 127.77±13.683 mmHg.
Diastolic blood pressure (DBP) was increased from 68.88±7.462 to 76.78±9.565 mmHg.
Mean blood pressure (MBP) was increased from 84.13±7.489 to 93.78±9.703, an increase of 11,47%. Blood pressure was increased less than between T25 and T120.
After the discharge of CO2 inflating, blood pressure was increased slightly and less, then progressive stability compared to the time of operation; high blood pressure was at the time of extubation due to irritation, blood pressure at recovery was lower than blood pressure at the time of operation (Figure 2).
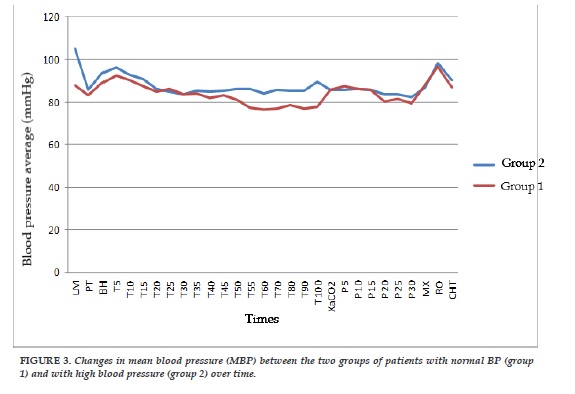
The mean blood pressure (MBP) in the two groups of patients was decreased at operation; at the time of starting CO2 inflation, MBP was increased dramatically between T5 and T25. The highest increase was in T5 with group 1 was 83.22±7.014 to 92.23±9.006 mmHg, or increased by 10.83%; for group 2 was 85.59±8.093 to 96.25±10.393 mmHg, or increased by 12.45%.
From T30, MBP in both groups was increased less and stable; after the time, MBP was increased slightly then decreased, increasing at the time extubation. In group 1, MBP was progressed toward MBP at baseline; in group 2, MBP at recovery was lower than MBP at baseline.
DISCUSSION
General characteristics of the patients
Age, gender of patients
Of the 86 patients studied, the youngest and the oldest were 22 and 73 years, divided into three age groups: 18 to 39 years old (37.21%); 40-59 years old (32.56%); ≥60 years old (30.23%). Three age groups were fairly uniform rates. Current laparoscopic surgery is performed on many different ages from young to old person. For gender: male was 37/86 patients, accounting for 43.02%; women was 49/86 patients, accounting for 56.98%.
The difference in male-female ratio was due to the fact that 10 patients with ovarian cysts were selected for the study.
Health status, condition and history of patients before surgery
The patients had study criteria for this study included patients without severe respiratory and cardiovascular diseases. The results obtained with the preoperative status of the patient were as follows: 68.60% of patients with ASA I (59 patients); 31.40% patients with ASA II (27 patients).
The condition of the patients was the normal general condition was 69.78% (60 patients); 5.81% (5 patients) underweight; 18.60% (16 patients) obese; 5.81% (5 patients) was obese with grade 1 and no one with obese of grade 2, 3.
Patient's history of surgery: the majority of patients underwent surgery had the healthy history of 63 patients (73.26%), 8 patients had hypertension (9.30%), 8 patients with gallstones (9.30%), 5 patients with gonorrhea (5.81%), 2 diabetic patients (2.33%). These conditions were mild, stable under treatment and could not affect the results of the present study [4-7].
Changes in pulse and blood pressure in patients undergoing laparoscopic surgery with CO2 pumping into the peritoneal cavity
The pulse was sharply decreased from T5 to T25; the smallest pulse was at T20; pulse was decreased from 76.85±7.630 to 67.05±10.396 beats/min, or was decreased 12.75%. The pulse was less changing and more stable from T30 to T120. After gradual discharge of CO2 pumping, there was a sharp increase of pulse due endotracheal extubation excitation and gradually progressed to the pulse at the time of surgery when the patients were transferred to recover room.
Among 86 patients in the present study, there were 34 patients with pulse below 60 times/min including 19 patients with pulse reduction to 51-59 times/min. There was 15 patients with a decrease of pulse ≤50 times/min. Patients with a reduction of pulse ≤50 times/min were treated with Atropin injections at a dose of 10 mcg/kg and 100% effective immediately after the injections, and the patients’ pulses were returned within normal limits. This finding is consistent with that of Ton et al. [8]: significant reduction in heart rate after CO2 inflation, 29.6% of cases had to use Atropine due to the pulse less than 50 times/min. The pulses were significantly slower before and after first 15 minutes of inflation and slight increased at the end of surgery.
The systolic blood pressure (SBP), mean blood pressure (MBP), and diastolic blood pressure (DBP) were lower at the time of surgery compared to the time of pre-surgery due to the effect of anesthesia. From the time of initiation of CO2 pumping, blood pressure starts to increase. Blood pressure was high in the period from T5 to T20; MBP was highest increased from 84.13±7.489 to 93.78±9.703 mmHg in T5, or increased of 11.47%. Blood pressure was increased less in the range of T25 to T120. After discharge of CO2, blood pressure was increased slightly; blood pressure was increased strongly at the time of extubation due to the excitation. At the time of recovery, blood pressure was gradually stabilized to that at surgery. This finding was consistent with Nguyen et al. [9,10]: MBP after 10 minutes of inflating was higher than before CO2 inflating with an average increase of 13.5 ±6.63 mmHg.
CONCLUSION
The pulse was greatly reduced from T5 to T25, the smallest pulse at T20. In the present study, there were some patients with the pulses very slow. However, they were recovered at normal limits after Atropin injection. The patients’ pulses were gradually increased after deflation and stabilized gradually to the value of the time of operation. Patients' blood pressures were increased during the first 20 minutes of CO2 inflation, the average increase of blood pressure was at T5. Blood pressure was increased less and stabilized from T25 to T120, after CO2 discharge.
CONFLICT OF INTEREST
The authors declare no conflict of interests for the present study.
REFERENCES
1. h t t p : / / w w w . v u s t a . v n / e n / n e w s / Thong_tin_Su_kien_Thanh_tuu_KH_CN/ Phau_thuat_va_phau_thuat_noi_soi_33594.html.
2. Department of Anesthesia, Hanoi Medical University. Anesthesia in Laparoscopic Laparoscopy. Anesthesia Lecture, Medical Publishing House 2002, p. 311- 318.
3. Huynh Thi Binh et al. Clinical Technique for Anesthesia, Medical Publishing House, 2004;Vol. 31-32.
4. Nguyen Van Chung. Anesthesia for Resuscitation for Laparoscopic Laparoscopy. Anesthesia Fundamental Anesthesia, Medical Publishing House, 2011;290-307.
5. Tran Binh Giang and Ton That Bach. Laparoscopic Laparoscopic Surgery, Medical Publishing House, 2012; 423.
6. Le Thi Viet Hoa. Monitoring and care of patients with mechanical ventilation, 01/03/2018, chuabenh.net / hoi-suc-cap-cuu / theo-do-va-cham-soc-benh -nhantho-may.html.
7. Hayel Gharaaibeh. Anaesthetic management of laparoscopic surgery", Eastern Mediterranean Health Journal, 1998;185-188.
8. Ton That Quang et al. Clinical characteristics and anesthesia for resuscitation in endoscopic ovarian cysts with intraperitoneal ovary pump", Medical Research, HCMC Medical Publishing House Ho Chi Minh City, 2011; 111-140.
9. Nguyen Manh Hong and Cong Quyet Thang. Anesthesia for Resuscitation in Laparoscopy, Huu Nghi Hospital in Hanoi; 2008.
10. Viale. J-P. (2007), "La ventilation peropératoire", Congrès national d'anesthésie et de resanimation. Les Essentiels, 2007;303-313.

FIGURES - TABLES

REFERENCES
1. h t t p : / / w w w . v u s t a . v n / e n / n e w s / Thong_tin_Su_kien_Thanh_tuu_KH_CN/ Phau_thuat_va_phau_thuat_noi_soi_33594.html.
2. Department of Anesthesia, Hanoi Medical University. Anesthesia in Laparoscopic Laparoscopy. Anesthesia Lecture, Medical Publishing House 2002, p. 311- 318.
3. Huynh Thi Binh et al. Clinical Technique for Anesthesia, Medical Publishing House, 2004;Vol. 31-32.
4. Nguyen Van Chung. Anesthesia for Resuscitation for Laparoscopic Laparoscopy. Anesthesia Fundamental Anesthesia, Medical Publishing House, 2011;290-307.
5. Tran Binh Giang and Ton That Bach. Laparoscopic Laparoscopic Surgery, Medical Publishing House, 2012; 423.
6. Le Thi Viet Hoa. Monitoring and care of patients with mechanical ventilation, 01/03/2018, chuabenh.net / hoi-suc-cap-cuu / theo-do-va-cham-soc-benh -nhantho-may.html.
7. Hayel Gharaaibeh. Anaesthetic management of laparoscopic surgery", Eastern Mediterranean Health Journal, 1998;185-188.
8. Ton That Quang et al. Clinical characteristics and anesthesia for resuscitation in endoscopic ovarian cysts with intraperitoneal ovary pump", Medical Research, HCMC Medical Publishing House Ho Chi Minh City, 2011; 111-140.
9. Nguyen Manh Hong and Cong Quyet Thang. Anesthesia for Resuscitation in Laparoscopy, Huu Nghi Hospital in Hanoi; 2008.
10. Viale. J-P. (2007), "La ventilation peropératoire", Congrès national d'anesthésie et de resanimation. Les Essentiels, 2007;303-313.
ARTICLE INFO
DOI: 10.12699/jfvpulm.9.28.2018.29
Conflict of Interest
Non
Date of manuscript receiving
Date of publication after correction
Article citation
Le Van T, Ta Thanh H. Study on the impact of CO2 inflation on cardiorespiratory system in patients having endoscopy surgery. J Func Vent Pulm 2018;27(9):29-34.



Copyright: jfvpulm.com